
"Cases" are undoubtedly the most reported metric with respect to COVID-19. Simply googling the word is enough to send one down a rabbit hole of fear-driven news. In this post, we seek to examine how labs test for COVID-19 positive "cases" and what to make of "case" statistics.
How do health officials test for COVID-19? For the past 8 months, the predominant method has been to use a lab technique called the reverse transcription polymerase chain reaction (RT-PCR) test.
Just as many of you may have experienced, this test requires a nasal or throat swab, from which the rtPCR test is used to rapidly make millions to billions of copies of existing RNA in your sample. The test amplifies existing RNA by "cycling". Each cycle amplifies the RNA in an exponential fashion as shown here:

The number of times your rtPCR test cycles is VERY IMPORTANT. This is called the "cycle threshold" (cT).
After this amplification process is complete, labs analyze your sample to see if they can find strands of COVID-19 RNA. If they do, you have just tested positive for COVID-19.
Why does this matter? An rtPCR test with too large a cycle threshold (cT) will make your test too sensitive. It will amplify tiny traces of dead, non-contagious virus RNA that is not infectious. Nonetheless, you will still be labeled as a positive case.
No matter what your opinions are on the New York Times, this is a solid article explaining this problem:



Let me repeat that: up to 90% of who test positive for COVID-19 are likely not contagious and do not need to isolate or submit to contact tracing.
This should be a national scandal.
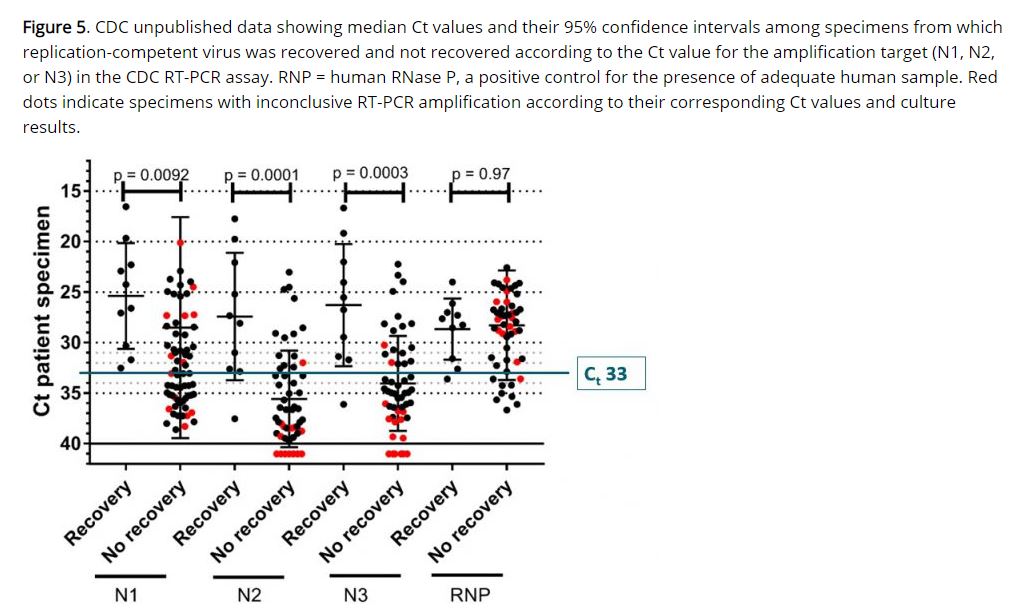
The CDC's own calculations indicate that it is almost impossible to detect/recover any live/infectious virus from a sample with a cycle threshold above 33. Because of the exponential nature of PCR amplification, this is a VERY different value than the standard 37-40 cycles being used across the country by several orders of magnitude.
This French IHU group goes even further, estimating that only 3% of COVID-19 rtPCR "positives" at a cycle threshold of 35 yield live virus upon culture.

From the paper: "Several works published recently and based on more than 100 studies attempt to propose such cut off for cT value and duration of eviction with a consensus at approximately cT > 30 and at least 10 days"
Again, a cT of 30 is VERY different from a cT of 37 to 40.
The following study lends credence to the previous French paper by demonstrating that if you no longer test positive 10 days from symptom onset at a cT of 30, you are very likely not infectious.

Can we confirm such high cT values across the board? Let's look at some of the manufacturer information/recommendations regarding these rtPCR tests.

Sensitivity is defined as the proportion of positives that are correctly identified. In order to achieve the highest possible sensitivity rating for their tests, manufacturers recommend high cT cutoffs consistently pushing 40.
As we've examined, the problem here is that not every "positive" represents an actual infectious/sick patient. We are merely scraping and amplifying tiny traces of dead non-contagious (non replication competent) RNA and classifying these people as positive cases.
This is not a new concern. Here's another paper discussing the problem back in April.

What is completely new however, is our bizarre indifference to the high cycle threshold problem of PCR testing. As the following paper details, we were certainly concerned about such problems and the consequences of rampant false positives in previous epidemics. What changed?

Are every nation's leaders and experts simultaneously making the same mistake? Is it an international conspiracy? Something in between?
I want answers and so should you.
Comments
Post a Comment